This isn't a technology trend to watch from a distance. It's an operational problem with practical solutions available right now.
This guide covers where AI delivers measurable impact in pharmacy workflows, how it differs from traditional pharmacy software, how to build an implementation roadmap, and how to keep pharmacists in control throughout. Whether you run an independent, community, specialty, or mid-market health system pharmacy, the principles apply.
Key Takeaways
- AI and automation reduce manual touchpoints across prescription processing, prior authorization, inventory, billing, and patient communications
- Target high-volume, repetitive tasks first — trying to automate everything at once rarely works
- AI supports pharmacist decision-making; human-in-the-loop design is non-negotiable
- Successful implementation starts with data readiness, clear KPIs, and a phased pilot before scaling
- The right implementation partner maps workflows before deploying any software — adoption depends on it
The Real Cost of Manual Pharmacy Workflows
Where the Time Actually Goes
In global mobility and HR operations, administrative overhead quietly consumes the majority of a team's working hours. Case managers chase document checklists. HR coordinators manually track visa expiration dates across spreadsheets. Immigration coordinators re-enter the same employee data across three separate systems. Skilled work — the kind that requires judgment and expertise — gets pushed to the margins.
This is a workforce utilization problem. When your most experienced staff spend the bulk of their time on tasks that don't require their credentials, you're leaving operational capacity unused every single day.
The strain compounds quickly:
- Teams handling 50+ active cases per coordinator report routine errors in status tracking and deadline management
- Manual data handoffs between HR, legal, and payroll create compounding delays at each transfer point
- Onboarding timelines stretch when immigration milestones aren't automatically flagged or escalated
- Burnout follows — and turnover in specialized mobility roles is expensive to recover from
The Downstream Cost of Manual Errors
Manual workflows don't just drain time — they create compliance risk. A missed visa expiration, a late I-9 correction, or a misfiled LCA can trigger penalties ranging from $2,500 to over $35,000 per violation under USCIS and DOL enforcement. Audit exposure compounds when records aren't consistently maintained.
Beyond regulatory risk, manual errors erode trust. Employees navigating international assignments or work authorization processes expect accuracy and speed. A dropped task or a delayed filing affects their ability to work — and reflects directly on the company sponsoring them.
Automation Isn't About Cutting Headcount
Automation in mobility operations isn't a staffing reduction strategy. It's a capacity expansion strategy. The same team currently struggling to keep pace with case volume can handle far more — with fewer errors — when they're not manually re-entering data, cross-referencing spreadsheets, or managing routine status updates by hand.
That's the operational shift AI-powered workflow tools make possible: not replacing expertise, but freeing it up for the work that actually requires it.
Where AI & Automation Are Transforming Pharmacy Operations
Prescription Intake and Verification
Traditional prescription verification requires a pharmacist or technician to check each incoming order against patient allergy history, current medications, and dosing guidelines — manually, sequentially, every time. AI changes the sequence without removing the pharmacist.
Modern AI-assisted verification tools read incoming prescription data, cross-reference patient history, flag dosing anomalies and drug interactions, and surface a prioritized review queue. The pharmacist still makes the call — they're just working from a pre-filtered list of cases that actually need their attention, not processing every routine refill from scratch.
The accuracy case is compelling: robotic dispensing systems have reduced unprevented dispensing errors from 0.015% to 0.002% — roughly an 87% reduction — in peer-reviewed trials.
Prior Authorization Automation
Prior authorization is where administrative burden becomes patient harm. The 2025 AMA Prior Authorization Physician Survey found that practices complete an average of 40 PAs per week, consuming 13 staff hours. Ninety-five percent of physicians say PA causes care delays. Seventy-nine percent report treatment abandonment as a result.
AI addresses this by identifying payer requirements automatically, gathering supporting documentation proactively, and initiating authorization workflows before they become bottlenecks. One academic medical center pharmacy study found PA completion time dropped from a mean of 20.9 days (when handled by the provider's office) to 1.9 days when managed by pharmacy staff with structured workflows.

Inventory and Supply Chain Intelligence
Machine learning forecasting tools analyze historical prescription patterns to predict restocking needs, reduce stockouts, and minimize medication waste. For pharmacy operators, this connects directly to cash flow: excess inventory ties up capital, shortages create emergency purchasing at premium prices, and expired medications represent pure loss.
ML-driven inventory tools improve purchasing decisions by replacing instinct-based reordering with pattern-based demand forecasting.
Billing, Documentation, and 340B Compliance
Specialty pharmacy billing and 340B compliance are areas where manual errors carry serious consequences. In FY2025, HRSA audited 115 covered entities and 49% received adverse findings — violations spanning diversion, duplicate discounts, and database inaccuracies.
AI automates clinical service billing, generates audit-ready documentation, and maintains continuous compliance logs that manual processes can't reliably sustain. For 340B-participating pharmacies, automated tracking is operational risk management.
Patient Communications and Medication Adherence
High-volume, low-complexity phone interactions — refill reminders, insurance status queries, appointment follow-ups — absorb staff time that compounds across thousands of patient touchpoints monthly. AI-powered outreach handles this tier of communication at scale.
A 2025 BMJ Open Quality study found that a digital medication refill system improved adherence from 51.3% to 90% among elderly hypertension patients while reducing medication oversupply from 42.5% to 7.7%. The clinical and operational impact reinforce each other.
AI vs. Traditional Pharmacy Software: What Actually Changes
Rule-Based Systems vs. Adaptive AI
Traditional pharmacy management systems execute predefined logic. A drug interaction alert fires when two specific medications appear together — because someone programmed that rule. The system can't distinguish between a routine combination and an unusual case; it treats both identically.
AI systems don't rely on exhaustive rule sets. They detect non-linear patterns across medication regimens, patient histories, and clinical data — identifying risks that rule-based systems would miss because no one thought to write that specific rule. Per ASHP's 2024 analysis, ML-based clinical decision support represents a meaningful evolution beyond traditional if-then alert logic.
Processing Unstructured Data
One of the most practical differences: AI can read inputs that traditional systems can't. Handwritten prescriptions, faxed forms, and voicemail messages all contain clinical information that currently requires a human to extract and re-enter. AI-driven OCR and NLP tools automate this extraction — not perfectly (handwritten prescription AI currently achieves around 81% exact match accuracy), but well enough to sharply reduce manual transcription volume while flagging edge cases for human review.
The Integration Layer
AI doesn't replace your pharmacy management system — it sits alongside it. Connecting AI tools to existing PMS platforms, EHRs, e-prescribing networks, and billing systems via APIs or HL7/FHIR standards is where integration pays off. Approximately 90% of prescriptions are now processed electronically, which means the data infrastructure for AI integration largely exists. The gap is usually configuration and connectivity, not raw data availability.
Point solutions vs. workflow orchestration: Many vendors offer narrow automation tools — phone bots, OCR for prescriptions, standalone prior auth tools. Each can deliver value in isolation, but the real efficiency gains come when they connect. Starting narrow is fine — just plan from the start for how isolated automations will link into a cohesive workflow.
How to Build a Pharmacy Automation Roadmap
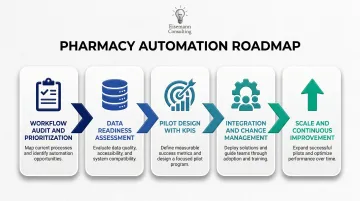
Step 1: Workflow Audit and Prioritization
Before evaluating any tool, map your current workflows. Identify where manual touchpoints are highest, where errors are most costly, and where automation would free the most staff time. The McKinsey framework for healthcare automation identifies the best candidates as repetitive, rule-based, high-volume tasks — roughly 33% of provider tasks fall into automatable categories using current technology.
Start with the obvious targets: prior authorization processing, refill approvals for stable chronic conditions, and outbound adherence calls. These offer the fastest ROI with the lowest implementation complexity.
Step 2: Data Readiness Assessment
AI tools perform only as well as the data feeding them. Before piloting any AI solution, assess:
- Structured access to patient medication history
- Clean, consistent medication records in your PMS
- API availability from your PMS or EHR
- HIPAA-compliant data governance policies and role-based access controls
Outdated pharmacy systems without modern API connectivity are a known barrier to AI adoption. If your PMS can't talk to external tools, that's the first problem to solve.
Step 3: Pilot Design with Defined KPIs
Scope your pilot carefully. Automating refill approvals for a single drug category or launching outbound adherence calls for one patient cohort is a better starting point than attempting broad implementation.
Track these KPIs from day one:
- Error rate reduction (pre/post)
- Time-per-task for automated vs. manual processing
- Prescription turnaround time
- Pharmacist intervention rate on AI-flagged items
- Patient satisfaction scores for automated touchpoints
Step 4: Integration, Testing, and Change Management
Technical integration — connector setup, data mapping, parallel validation — matters, but change management matters more. Pharmacists and technicians who weren't involved in tool selection will find reasons to work around it.
Build adoption from the start by:
- Involving clinical staff in tool selection, not just deployment
- Validating AI outputs against manual processes before going live
- Documenting override and escalation protocols before the first edge case appears
Step 5: Scale and Continuous Improvement
Full deployment requires feedback loops, not just a go-live date. Pharmacist corrections to AI recommendations should feed back into model improvement over time. Track where the system escalates to human review most frequently — those patterns reveal where additional training or rule refinement is needed.

This is where workflow consulting expertise creates value that software vendors typically don't provide. Firms like Eisemann Consulting — which applies an AI-enabled, human-led approach across mid-market operations through engagements like its AI Automation Starter and Scalability Accelerator — map current-state workflows, identify integration gaps, and sequence implementations to build on each other.
A vendor deploys their product and moves on. For pharmacy teams without dedicated IT staff, that distinction often determines whether automation gets adopted or quietly abandoned.
AI-Enabled, Human-Led: Keeping Pharmacists at the Center
The Governance Principle
Every AI system in a pharmacy workflow should operate as an assistant, not a decision-maker. Pharmacists retain final authority. This is codified across all 50 states: licensed pharmacists must exercise professional judgment and perform final verification before any medication is dispensed.
In practice, human-in-the-loop design means:
- AI surfaces recommendations and flags risks; pharmacists approve or override
- Clear escalation rules define which cases require pharmacist review before proceeding
- Override protocols are documented and tracked — not just technically available
- No dispensing action occurs without pharmacist sign-off
In September 2025, the Joint Commission and Coalition for Health AI released the first national guidance on responsible AI adoption in healthcare, applying to over 22,000 accredited organizations. The guidance explicitly requires healthcare organizations to develop local validation policies, monitoring protocols, and human oversight structures. For pharmacy operations leaders, this framework is the starting point for any responsible AI implementation.
Building Staff Trust
Governance structures only work if staff actually use them. A 2026 survey of 405 pharmacists found that 56.3% hold positive attitudes toward AI adoption — a majority, but not a landslide.
The research is clear on what drives acceptance: accuracy alone doesn't build trust. Pharmacists need to understand how recommendations are generated, see evidence that the system handles edge cases appropriately, and receive training focused on interpreting AI outputs — not just navigating interfaces.
Explainability is non-negotiable. When a pharmacist can see why a case was flagged, evaluation is faster and more confident. Opaque reasoning eliminates the efficiency benefit entirely — every recommendation demands the same mental load as a manual check.
Audit Trail Requirements
Every AI-assisted decision needs a documented record: what the system recommended, what the pharmacist decided, and when. This protects the organization during payer audits and regulatory inspections. Under HIPAA's Security Rule, covered entities must implement audit controls that record and examine access to PHI — and that requirement extends to AI systems processing patient data. Design the audit trail into your implementation from day one — retrofitting it after go-live is significantly more disruptive and often incomplete.
Choosing the Right AI Automation Partner for Pharmacy Workflows
Pharmacy software and workflow automation consulting solve different problems — and confusing the two leads to expensive missteps. A software vendor deploys their product. A consultant maps your current-state workflows, identifies where automation fits your specific operations, sequences implementations so they build on each other, and ensures the technology gets adopted by the people using it daily.
For mid-market pharmacy operations teams without dedicated IT or automation staff, this distinction is critical.
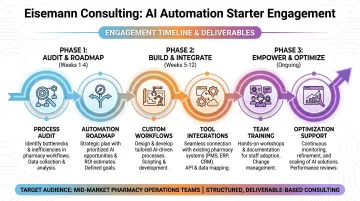
Eisemann Consulting's automation approach uses low/no-code platforms — Zapier, Airtable, Retool, and Make — built to deliver scalable workflows without requiring in-house IT infrastructure. The AI Automation Starter package (an $8,000 one-time engagement) includes a process audit, automation roadmap, three to five custom workflows, tool integrations, team training, and 30 days of optimization support.
For pharmacy operations teams beginning their automation journey, this structured entry point is designed to surface 10–20 hours of weekly savings without requiring technical staff to own the rollout.
For new clients evaluating fit, Eisemann Consulting also offers a free operational fix — identifying and resolving one workflow bottleneck within 72 hours, at no cost and no commitment. Limited to five businesses per month.
When evaluating any automation partner or software platform, assess:
- Integration compatibility with your existing PMS and EHR
- HIPAA compliance certifications and BAA availability
- Ability to pilot before committing to full deployment
- Transparent pricing with defined deliverables
- Ongoing support after launch — not just implementation
Frequently Asked Questions
Will AI replace pharmacists or pharmacy technicians?
No. AI automates routine, repetitive tasks — data entry, refill processing, prior auth documentation — so pharmacists can focus on clinical judgment, patient counseling, and safety-critical decisions. Human oversight remains a regulatory and ethical requirement at every stage of the dispensing process.
What pharmacy workflows are easiest to automate first?
High-volume, rule-based tasks offer the fastest ROI with the lowest implementation risk: refill approvals for stable medications, prior authorization data gathering, outbound adherence reminders, and inbound call triage. These deliver measurable time savings without touching complex clinical workflows.
How long does it take to implement AI automation in a pharmacy workflow?
Simple communication automation — outbound reminders, inbound call routing — can go live in weeks. Full workflow integration with PMS or EHR systems typically takes several months. A phased pilot approach reduces timeline risk and allows for course correction before full deployment.
How do I ensure HIPAA compliance when using AI in pharmacy operations?
Verify the vendor holds HIPAA compliance certifications and will sign a Business Associate Agreement. Implement role-based access controls, encrypt patient data in transit and at rest, and document the AI system's role in all audit trails — HHS OCR is actively enforcing HIPAA against organizations deploying AI without adequate PHI safeguards.
What ROI should I expect from pharmacy workflow automation?
Results vary by use case, but peer-reviewed benchmarks provide a reliable baseline:
- Robotic dispensing reduces dispensing errors by approximately 87%
- Digital refill systems have improved medication adherence from 51% to 90% in clinical studies
- McKinsey estimates healthcare administrative automation can reduce administrative costs by roughly 40%
Vendor claims tend to outpace these figures — hold partners to published benchmarks.
Do I need a large IT team to implement AI pharmacy automation?
No. Low/no-code platforms make meaningful automation achievable for pharmacy operations teams without dedicated technical staff. What matters most is clear workflow documentation before implementation and a phased approach that builds confidence before scaling.